
What the drive for universal health coverage misses
Inequality in care is today’s greatest health crisis
· 5 min
Image on right by aleksandarlittlewolf/Freepika
Opinion
By Gijs Walraven, Director for Health, Aga Khan Development Network
- SDG 3 aims to achieve universal health coverage (UHC) by 2030. The number of countries with poor coverage decreased from 55 in 2000 to eight in 2023, with the fastest progress in countries that were lagging most behind.
- But the pace has slowed. Too often, no care is being replaced with poor care. Stark disparities continue.
- We need to organise technology, knowledge and financial resources better to consistently serve the most disadvantaged.
Universal health coverage: built on an illusion
The global drive for UHC is not merely off-track; it is fundamentally flawed. Ten years after the United Nations endorsed accelerating UHC, and nearly halfway through our timelines to achieve the 2030 Sustainable Development Goal target, our conversation about UHC must shift from one of access to one of quality. Health service coverage has expanded in nations that were previously lagging, but this progress has been built on the illusion that simply providing access to health care will help us achieve equitable health care for all.
Global healthcare access: 2000 vs 2023
Universal Health Coverage Service Coverage Index, by countryHover over a country to see its UHC score
UHC Service Coverage Index measures access to essential health services on a 0–100 scale, covering family planning, maternal and child health, immunisation, and infectious and non-communicable disease treatment. It is SDG indicator 3.8.1.
The reality, however, is that “no care” is rapidly being replaced by “poor care”.
A joint report by the World Health Organization and World Bank confirms that global access to health services has improved substantially, but quality, continuity and resilience differ sharply. For billions around the world, UHC has become an empty promise. Many assumed that expanding coverage and removing user fees would automatically produce equity. Experience has shown that this is not the case.
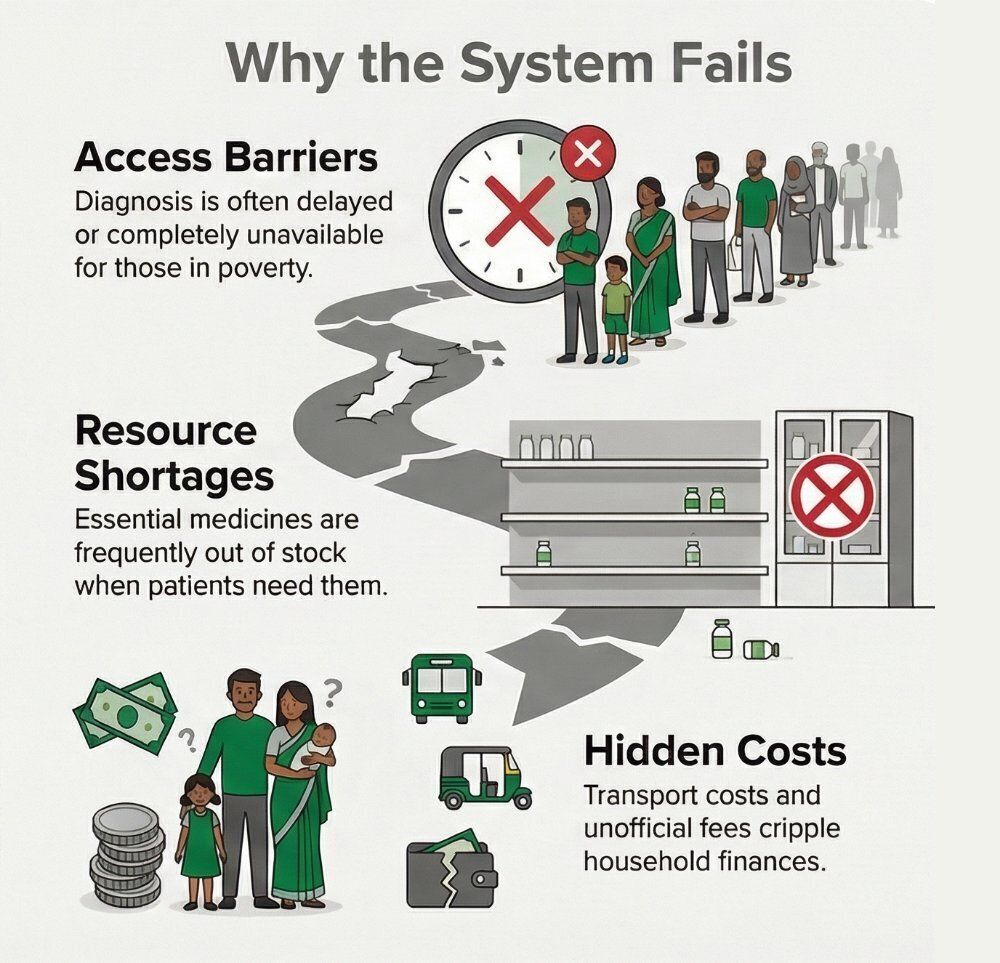
UHC now exists alongside deep inequities. Like Joseph, a poor patient may be formally insured. Like Fatima, they may be exempt from consultation fees. But their healthcare system still fails them when:
- diagnostics are unavailable or delayed;
- essential medicines are frequently out of stock;
- staff are overstretched, leading to inadequate or fragmented follow-up;
- referral hospitals charge informal fees; or
- out-of-pocket costs for transport, diagnostics and medicines remain catastrophic, crippling household finances.
Here, coverage is a victory for bureaucracy – but a defeat for the patient. The system meets UHC targets on paper but fails because quality breaks down along the care continuum. Equity must not be measured by how many people are “covered”, but by whether the system consistently delivers care of adequate quality to those who need it most.

Earlier, patients were described as lacking knowledge and facing financial constraints and geographic barriers. Today, they are more informed but poorly protected. Patients now know their rights and available treatments, but when systems fail to deliver, they lose trust in health providers.
At the same time, patient profiles themselves are changing. Chronic diseases like cardiovascular disease, diabetes and HIV are imposing long-term economic strain on healthcare systems, while multi-morbidity – infectious diseases layered with non-communicable diseases, mental health conditions and physical illness – is becoming more common. Health systems built on vertical, disease-specific programmes are structurally incapable of managing this complexity. As a result, patients are no longer simply excluded; they are included on unequal terms.
Systems, not programmes: the mandate for equity
Today, global health governance is marked by numerous but incoherent institutions, shifting donor priorities, weak accountability, misaligned policies and institutional silos. Poor-quality care inevitably follows. What we need is the ability to organise technology, knowledge and financial resources in ways that consistently serve the least advantaged.
A shift from programmes to systems that deliver equity could make a meaningful difference. This requires:
- Re-centering on Primary Health Care (PHC): this is the only way to scale up and provide equity. A family medicine approach can anchor care in longitudinal, trusted relationships, shifting the focus from episodic treatment to life-course management of risk, illness, recovery and care. It can be uniquely designed to manage diagnostic uncertainty and handle the multi-morbidity that defines the burden of disease today.
- Making quality non-negotiable: UHC without quality has reached its limits. We need minimum quality standards that apply to everyone, regardless of facility or geography. Investment must target diagnostics, supervision, referral and learning systems. Accountability must be about measurable health outcomes, not usage targets. Organisations like SafeCare, which measure and certify quality, as well as benchmark progress, offer critical tools to help drive more efficient and safer care.
- Building resilience to protect equity: a health system that collapses under stress – whether from a pandemic, climate event, or conflict – is inherently inequitable. Resilient systems that continue essential services, protect health workers and maintain supply chains are vital.
Innovation must prioritise the fragile
Innovations that reach high-need populations must be simple, publicly funded and designed for low-capacity environments. In remote northern Pakistan, where neonatal mortality is high, a low-cost integrated care kit is delivered directly to pregnant women via community health infrastructure, alongside evidence-based maternal and newborn interventions. This example shows how care can reach fragile settings effectively.
Simplified treatment protocols and rapid testing should be prioritised. Health service delivery for chronic conditions such as diabetes and cancer must be integrated and patient centred. Digital health also holds immense promise – but only if it reaches rural, older, poorer, undocumented, or low-literacy populations. Innovations must be designed to strengthen health systems and prioritise long-term outcomes rather than short-term humanitarian responses.
The bottom line is clear: we must stop seeing scaling up in fragile settings as “too risky”. These are precisely the environments where poor populations are most exposed to unsafe care and where innovation pipelines most often break down.
A political choice
UHC cannot rely on volatile aid, out-of-pocket payments and fragmented insurance schemes. It requires a commitment to progressive domestic financing and risk pooling that truly cross-subsidises the poor and incentivises quality-driven PHC. Equity requires intentional redistribution, not trickle-down coverage.
Ultimately, UHC is a political choice. Leaders must prioritise long-term population health and accountability to communities. Health service providers alone cannot deliver equitable health. Addressing the social and environmental determinants remains vital. By 2030, UHC must mean protecting everyone from avoidable suffering across the life course, regardless of income, gender, geography, religion, or crisis. Nothing less is acceptable for us to achieve a truly equitable and sustainable health system.